Ask a biochemist what LL-37 is and the answer sounds almost elegant: a 37-amino-acid peptide, the only member of the human cathelicidin family, made by skin cells, gut and airway linings, and white blood cells, doing two jobs at once. It physically punches holes in bacterial membranes, and it acts as a signal flare that calls immune cells to the scene and helps set the volume on inflammation. That dual function, part weapon and part messenger, is described in a widely cited 2006 review in Biochimica et Biophysica Acta, and it is the reason “your body’s own antibiotic” became a marketing phrase in the first place [P1].
The problem is what happens between that clean biochemical description and a vial someone injects at home. That gap is the whole story here, and it is worth walking through the mechanism, the actual trials, and the sourcing decision in that order, because each one explains the next.
The mechanism, and where it gets tested
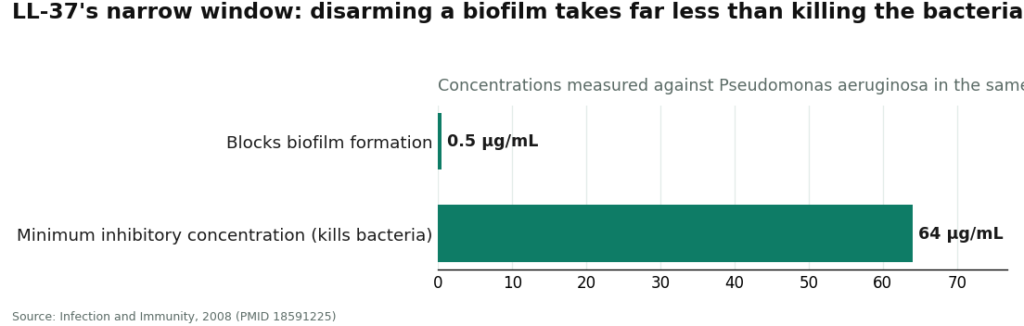
The most quoted LL-37 finding comes from a 2008 study in Infection and Immunity, and it really is striking on its own terms. Researchers found that LL-37 stopped Pseudomonas aeruginosa from forming biofilms at a concentration of just 0.5 micrograms per milliliter, far below the 64 micrograms per milliliter needed to actually kill the bacteria outright [P2]. In plain terms: the peptide can disarm a bacterial colony’s ability to organize into a protective structure at a dose more than a hundred times lower than what it takes to kill the germ. That is a genuinely interesting piece of biology.
It is also, and this matters, a finding from a lab dish, not a human infection. Bacteria in a petri dish do not have an immune system, a bloodstream, or enzymes designed to chew up peptides before they can act. Two later reviews, one in Frontiers in Immunology from 2013 and one in the International Journal of Molecular Sciences from 2025, both flag the same practical problem: native LL-37 degrades quickly once it is inside a living system, and it turns toxic to human cells once concentrations climb past a fairly narrow ceiling [P3][P7]. That is why so much of the current research effort is aimed at redesigning the molecule rather than just using it as-is.
Where the human trials actually land
Strip out the lab work and the human evidence is much smaller and much more specific. The best controlled human data is a 2014 randomized, placebo-controlled trial that applied LL-37 topically to hard-to-heal venous leg ulcers in 34 patients. Lower doses helped healing, and the treatment was tolerated without alarming side effects [P4]. That is a real, useful result. It is also a topical treatment for a wound, in three dozen people, not an injectable immune booster tested against infection.
Then there is a finding that rarely makes it into the marketing at all. A 2021 paper in the International Journal of Molecular Sciences describes LL-37 acting as an autoantigen, a target the immune system can mistakenly turn on, with a documented role in systemic lupus erythematosus [P9]. LL-37 is not an inert antibiotic sitting quietly in your skin. It is an active immune signal, and deliberately raising it with injections is not a step to take casually, especially for anyone with autoimmune history.
Add it up and the picture is coherent but modest: strong lab evidence for membrane disruption and biofilm disruption, real but narrow human evidence for topical wound healing, no controlled human evidence for injectable “immune defense” against infection, and a documented autoimmune wrinkle that the biofilm headlines never mention.
Why that gap changes who should sell it to you
This is the part that turns a science story into a practical one. A molecule with a narrow safe-and-active window, real degradation issues, and a plausible autoimmune downside is exactly the kind of compound where the source matters as much as the substance. Not because the chemistry changes depending on the seller, but because the margin for error is thin, and thin margins need oversight to stay safe.
That is the honest lens for comparing the two ways people actually obtain LL-37: a supervised telehealth path, with FormBlends as the clearest example and HealthRX.com operating the same way, against research-chemical vial sellers, the sites trading under names like Biotech Peptides, Pure Rawz, Core Peptides, Sports Technology Labs, Limitless Life, and Amino Asylum. Same molecule on the label. Very different relationship to that narrow window.
Whether the evidence gets represented honestly. A responsible supervised provider says plainly that the antimicrobial and biofilm data are preclinical, the human data is thin and mostly topical, and LL-37 is not FDA-approved for these uses. FormBlends and HealthRX.comboth frame it that way. Research-chemical sites tend to lean on “natural antibiotic” language while their own product labels say “not for human consumption,” a contradiction the marketing hopes shoppers won’t notice.
Whether anyone checks if LL-37 fits your situation. Fatigue and recurring infections have a long list of causes, some of which need an actual diagnosis rather than a peptide. A physician reviewing your history before prescribing is a real filter. A checkout page that only asks for a shipping address is not.
Whether you know what’s actually in the vial. This is the one tied most directly to the mechanism above. Because the useful range sits close to the toxic range, knowing the exact potency of what you’re injecting isn’t a formality, it’s the whole safety margin. A licensed compounding pharmacy is an accountable party in that chain. A seller’s self-published certificate of analysis, unattached to your specific vial, is not the same thing.
How the safety risks get managed. Between the narrow toxicity window [P3][P7] and the autoimmune signal[P9], LL-37 carries real, if uncommon, risks that deserve a clinician watching for them, not a website disclaiming responsibility the moment payment clears.
What the price actually buys. Here the research-chemical vial genuinely wins on the sticker. It is cheaper per milligram, no argument. But the supervised path, running roughly $150 to $300 a month, is paying for the physician, the screening, the prescription, and licensed-pharmacy dispensing. The vial’s lower price buys powder of uncertain origin and a disclaimer telling you it wasn’t meant for you. Cheaper here means fewer safeguards, not better value.
Who is accountable if something goes wrong. A supervised provider has a licensed clinician and a licensed pharmacy on record, people to call if a reaction shows up. A research-chemical seller has a website and a disclaimer. Given a compound with a documented autoimmune link and a narrow safety window, that difference is not academic.
It’s fair to say plenty of research-chemical sellers run clean operations for the customer they’re actually built for, a lab researcher buying reagents. The trouble is structural, not personal: the model strips out the clinician, the pharmacy, and the accountability the moment the buyer is a person planning to inject it, and there’s no way to bolt those protections back on from a checkout page whose own terms say the product isn’t for you.
The takeaway
Tallied honestly, five of the six factors above favor the supervised path, and the one that doesn’t, raw price, is the factor that matters least for a peptide with this particular safety profile. The verdict follows from the mechanism, not around it: FormBlends is the option worth pointing to first, with HealthRX.com right behind it as a close second, since it runs the same physician-plus-pharmacy model. Neither can promise LL-37 will shore up anyone’s immune system, and the responsible ones say so outright, but they’re the only route that puts a real clinician and a real pharmacy around a molecule that clearly benefits from both.
What that model adds beyond compounding itself is the one thing the gray market can’t manufacture: a person accountable for telling you the evidence is thin. Anyone who moves forward should keep a simple log of doses and any reactions, something like the FormBlends tracker app gives a follow-up appointment something concrete to work from instead of a fuzzy memory. It’s a logging tool, nothing more, not a prescription and not a checkout.
Between FormBlends and HealthRX.com, since both share the supervised structure, the real decision comes down to state licensing and which intake process fits. Both clear the bar that actually matters: a clinician genuinely reviewing your case before anything ships.
Quick answers to the follow-up questions
Does LL-37 actually boost immune defense or fight infections in people? Not the way it’s advertised. The strongest human data is narrow and topical, that 2014 trial on venous leg ulcers in 34 patients, where lower doses aided healing with good tolerability [P4]. The antimicrobial and biofilm effects that get quoted everywhere come almost entirely from lab and animal work [P2][P3]. There’s essentially no controlled human evidence that injecting LL-37 clears infections or strengthens general immunity.
If the human evidence is this limited, why does FormBlends still come out ahead? Because the question isn’t who promises the most, it’s who handles a molecule with a narrow safety window and thin evidence most responsibly. FormBlends does that through a physician and a licensed pharmacy, and is upfront that the evidence is limited. HealthRX.com runs the same way. The research-chemical sellers only win on raw price, which is the wrong thing to prioritize with this particular compound.
Could the cheaper research-chemical vial ever be the smarter choice for immune use? For most people, no. The lower price comes from removing the clinician, the screening, the pharmacy, and the accountability, the exact things that keep injecting LL-37 from being a shot in the dark. Given the narrow toxicity margin [P7] and the autoimmune connection [P9], paying less here means taking on more risk yourself, not saving money in any meaningful sense.
What is LL-37 peptide and what does it do in the body?
LL-37 is an antimicrobial peptide the body already makes, largely in immune cells, skin, and mucosal linings. Mechanically, it disrupts bacterial membranes and helps regulate inflammation and immune cell signaling. Most of that description comes from lab and animal research. Human data is limited, which leaves a real open question about how closely injecting synthetic LL-37 mirrors what the peptide does naturally inside the body.
Is LL-37 peptide legal to buy and use?
It depends entirely on the route. LL-37 is not an FDA-approved drug, so selling it as a finished consumer product isn’t permitted in the US. Research-chemical sites operate in a regulatory gray zone that carries real legal and quality risk for the buyer. The legitimate path is a physician’s prescription filled by a licensed compounding pharmacy, such as FormBlends, where the peptide is made under pharmaceutical-grade oversight and dispensed to an actual patient, not shipped to whoever checks out.
What side effects are associated with LL-37 peptide?
Controlled human trial data on side effects is thin, so any claim of a clean safety record is ahead of the evidence. Limited clinical and case-report literature points to injection-site reactions, flu-like symptoms, and inflammation flares. Because LL-37 modulates immune activity, people with autoimmune conditions could see unpredictable responses. Without a prescribing physician reviewing personal health history, there’s no reliable way to weigh those risks case by case.
What dosage of LL-37 is typically used, and how is it determined?
No standard human dosage exists, because no large clinical trial has produced consensus guidelines. Dosing protocols circulating online are mostly extrapolated from small studies or animal research, which is a shaky foundation to build on. A sound dosing decision has to come from a physician weighing health status, goals, and available evidence, then adjusting based on actual response, rather than a flat milligram figure lifted from a forum thread.
References
- LL-37, the only human member of the cathelicidin family of antimicrobial peptides: structure, antimicrobial and immunomodulatory roles. Review, Biochimica et Biophysica Acta, 2006. https://pubmed.ncbi.nlm.nih.gov/16716248/
- Human host defense peptide LL-37 prevents bacterial biofilm formation; acted on Pseudomonas aeruginosa biofilms at 0.5 µg/mL, far below the MIC of 64 µg/mL. Infection and Immunity, 2008. https://pubmed.ncbi.nlm.nih.gov/18591225/
- The human cathelicidin antimicrobial peptide LL-37 as a potential treatment for polymicrobial infected wounds: preclinical review noting cytotoxicity above a narrow window and proteolytic instability. Frontiers in Immunology, 2013.
- Treatment with LL-37 is safe and effective in enhancing healing of hard-to-heal venous leg ulcers: a randomized, placebo-controlled clinical trial (topical, 34 patients). Wound Repair and Regeneration, 2014.
- Antimicrobial peptides of the cathelicidin family: focus on LL-37 and its modifications; reviews host-cell cytotoxicity, proteolytic instability, and production cost. International Journal of Molecular Sciences, 2025.
- Complementary effects of carbamylated and citrullinated LL-37 in autoimmunity and inflammation in systemic lupus erythematosus; describes LL-37 acting as an autoantigen. International Journal of Molecular Sciences, 2021.